Posts Tagged covid
Science should dictate policy, not the other way around.
Posted by Nick Bennett MD in Antivax, Nick Bennett MD, Public Health, Vaccines on July 2, 2024
It’s taken me a little while to put virtual pen to paper in response to the appalling report from Reuters that revealed how an official US-government-sanctioned campaign set out to deliberately undermine COVID vaccination efforts in the Philippines.
Through phony internet accounts meant to impersonate Filipinos, the military’s propaganda efforts morphed into an anti-vax campaign. Social media posts decried the quality of face masks, test kits and the first vaccine that would become available in the Philippines – China’s Sinovac inoculation.
Reuters
The program, which apparently ran from 2020 through the end of the Trump administration and months into 2021, was a deliberate act of propaganda to undermine the influence of China on the global COVID vaccine stage (which the USA was not contributing to at all at the time). While Americans were “not targeted” by the misinformation, that specifically set out to disparage and undermine the Sinovac vaccine that was in widespread use in that region at the time, there cannot be any doubt that the lives of locals were placed at risk. As an infectious disease specialist who has dealt with antivaccine misinformation for all of their professional career, this is simply unacceptable to me. Regardless of the relative merits of one vaccine over another, or the petty machinations of the political regimes, during a global pandemic it is an abject failure of humanity to deliberately place other human beings in harm’s way.
This isn’t the first time that vaccines have been used as tactical tools – in the hunt for Bin Laden the CIA used a hepatitis vaccine program to collect DNA from children in an attempt to discover links to the terrorist in hiding. When the ruse became public, vaccine workers (even those with nothing to do with the program) were targeted and the polio eradication campaign stalled, with effects that have taken over a decade to even start to undo.
In response to the Pentagon’s efforts to undermine China, Filipino vaccine rates were woefully low, to the extent that the Government had to threaten jail for those who refused vaccination. When the US was approaching herd immunity at 65% coverage, in June 2021 the Philippines had only about 2% of their population immunized.
It takes a special kind of heartless disregard for science, and the welfare of other human beings, to promote this kind of act and go along with it. I suppose should we expect anything less, coming from a political leader who downplayed the seriousness and very existence of the problem and then politicized masking and social distancing, even as they sent protective equipment to their political allies. After vaccines became widely available, the anti-science mindset among Republicans was responsible for a 43% higher rate of excess deaths compared to Democrats in Florida and Ohio.

Arguably, deliberately undermining vaccine programs for political gain is tantamount to poisoning a water supply, which is literally a war crime. I cannot overstate how upset I am about this entire story – we as the experts have a hard enough time educating a scared and skeptical public about the measures that we are recommending to literally save them from themselves, without having our work attacked and undone by the powers that be.
Should I get the COVID vaccine?
Posted by Nick Bennett MD in Uncategorized on November 22, 2020
TL:DR – Yes.
*Tap tap* – is this thing still on? It’s been a while.
The recent slew of data coming out from Pfizer and Moderna about their respective COVID vaccines has prompted a LOT of discussion about their utility, safety, and efficacy. I’ve had friends and family hit me up for my opinion through social media, private messages, and phone calls, and the truth of the matter is there’s a 50% chance I’ve already got a vaccine, and if I haven’t the company is looking to provide it to those in the placebo arm. Yes, I’m in a COVID vaccine clinical trial – the science and need is compelling.
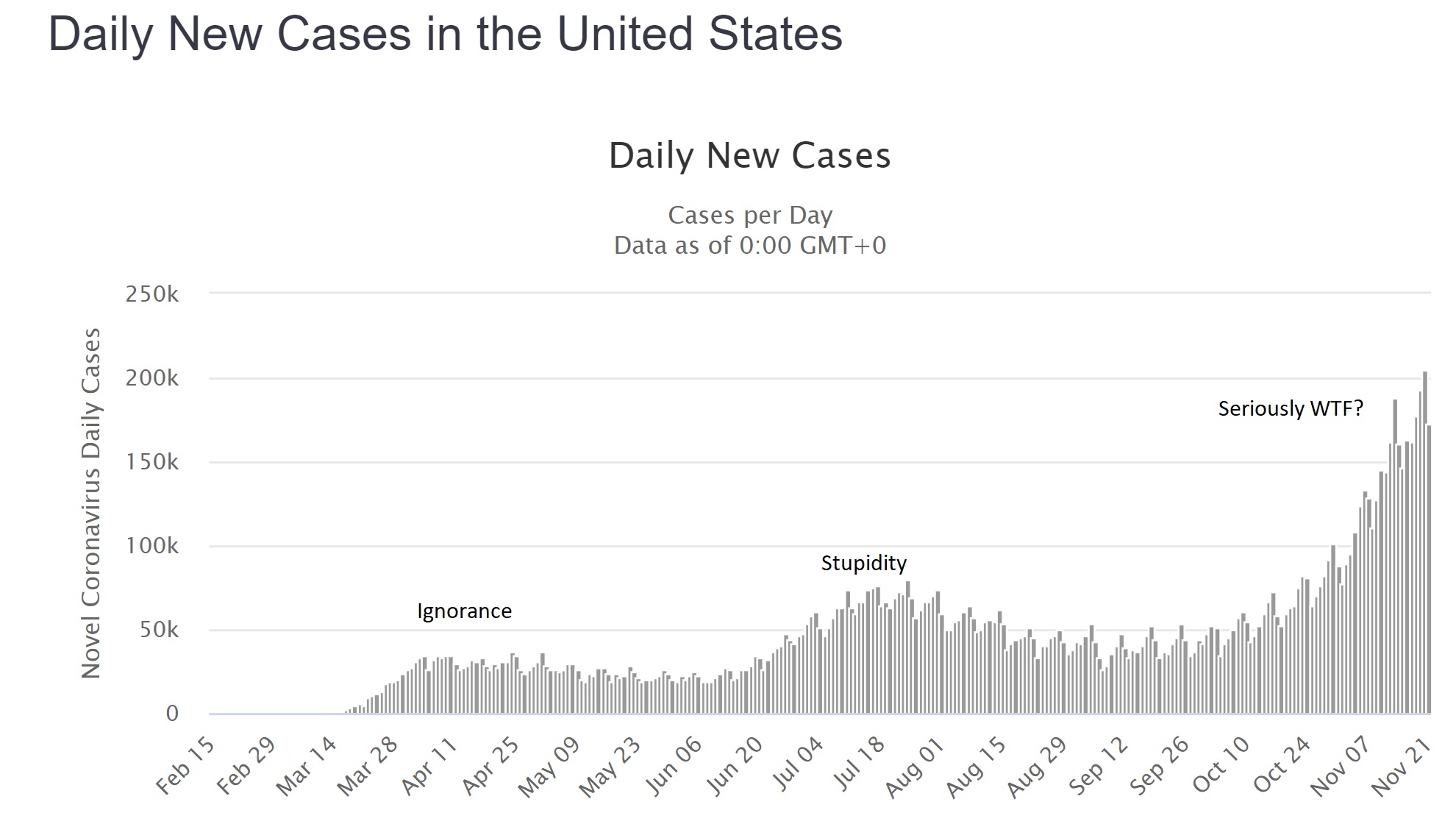
The global cases of COVID continue to climb with over 58 million worldwide as of today, of which about 12.5 million are in the US. Facing an accelerating “third wave” of cases of around 200,000 new reports and 2,000 deaths from COVID every day, there is no end in sight. This isn’t a hoax, it isn’t a “plandemic” or some other bizarre conspiracy theory, and it didn’t go away after the election – what we are dealing with is a predictable novel infection, likely zoonotic, the effects of which have been made worse by a series of abject failures in public health and education. I’m not going to debate that – it’s a matter of fact. Trolls will have their comments happily deleted, because I don’t argue with people who are wrong.
Having failed miserably to prevent the spread of this infection through such simple measures as staying home and covering faces, we now appear to have little option but to have faith in a vaccine of some kind. Herd immunity will otherwise cost millions of lives and probably trillions of dollars in lost productivity and economic output. The “low” mortality of 2-3% for COVID-19 is not low at all (the risk of death from a car crash is half of one percent, yet no-one in their right mind would recommend deliberately crashing their car…), and in any case the long-term effects of the infection on peoples’ health is likely to impact society for years to come. The fastest, safest way to stop the virus is through vaccination.
There are two vaccine candidates that have made headlines recently, both with similar technologies and claims of effectiveness, so for the sake of simplicity I’m going to talk about them generically. It seems likely that one or both of them will be approved by the FDA.
The vaccines use a “new” technology called “messenger RNA” or “mRNA”. The concept of an mRNA vaccine is not in fact new, and they have been researched for years. mRNA is entirely natural – every cell in your body contains some – very simply it is used as a go-between (a messenger…) from the genes coded within your DNA to the ribosomes where proteins are made. mRNA has a very specific structure – a linear molecule consisting of a mixture of 4 different nucleotides (adenine, cytosine, guanine and uracil) with a cap and a tail to ensure that the code is translated correctly and that other bits of RNA aren’t used accidentally. After the mRNA molecule is translated it is simply degraded and the individual nucleotides are recycled.
In theory, and apparently in practice, the use of an mRNA molecule as a vaccine would have several advantages. Most vaccines can be divided into one of two types: killed (or subunit) and live-attenuated. mRNA vaccines manage to combine the positive aspects of BOTH kinds, but the negative aspects of NEITHER. Allow me to explain.
In a normal viral infection the virus has to invade the body and evade the immune response, then infect a host cell. Viruses cannot replicate without a host cell, but in many instances the virus infection damages the cell function such that the host is affected and becomes sick. A virus that successfully infects a cell can take over the cellular functions, produce viral mRNA molecules, and force the cell to produce viral proteins. Cells though have several lines of defense, from producing chemicals called “interferons” that combat viral infection, to presenting viral antigens on their surface to the immune system (specifically, CD8+ T lymphocytes). Whether through the “innate” immune response like interferons, or through the “adaptive” immune response like T cells, nearly all of the time the host is able to successfully contain and clear a viral infection.
With a live-attenuated vaccine the goal is to mimic the natural infection, but without putting the host at risk of getting sick. The vaccine is usually made in such a way that the virus is defective and some aspect of its life-cycle is damaged – this means that the virus will still infect a cell and will still present its proteins to the host T cells, but the host simply won’t get as sick as they would with a wild-type infection. The result is often a VERY effective immune response that can last a lifetime after a single dose of vaccine, although sometimes boosters are given a few years later. Examples are measles, mumps, rubella, yellow fever, and oral polio vaccine.
Killed vaccines on the other hand use only “bits” of the virus, usually proteins that make up the capsid or outer membranes that are targets of the host immune response in natural infection. The hope is that by showing the host the purified proteins the immune system will produce a response that will recognize the virus should it try to infect the host in the future. The downside of these vaccines is that the type of immune response is slightly different, as the proteins are not presented from *inside* the cell. As such, the T cell responses are typically less, but instead there is a strong antibody response. Antibodies are very good at recognizing and neutralizing infections outside of cells, but of course since viruses replicate inside cells the real immunity actually depends on those CD8+ T cells. As such, killed vaccines often need multiple doses to be effective, and may not provide as much protection as the live vaccines would. Their advantage though is safety – there is literally no way for a killed vaccine to give the host an infection, whereas live-attenuated vaccines CAN cause disease if the host has an immune deficiency or if the virus mutates.
Looking now at mRNA vaccines it would seem as if they have the benefits of live-attenuated (internal protein production and presentation to T cells) AND the benefits of killed vaccines (no risk of causing infection in the host). In addition, despite the conspiracy theories you may read about online, there is no risk that the vaccine “becomes part of you” since there isn’t a mechanism for it to do so. Furthermore, a COVID-19 mRNA vaccine is an even better deal. The virus that causes COVID-19 has two very problematic aspects to it – firstly, it directly and significantly decreases that innate interferon response that is intended to stop the virus becoming established. This is likely because it evolved in bats, which have inherently high levels of interferon. In a human host, this virus is able to suppress our immune system very effectively, so that an otherwise mild infection is far more serious. Secondly, the adaptive immune responses (especially the T cell responses) in patients with COVID are also suppressed. Very early on it was obvious that the sickest patients with COVID had low number of lymphocytes, and over time we have come to realize that this also led to decreased adaptive immune responses against the virus. It seems that without the normal early response to infection, the host immune system is led awry, causing a dramatic, abnormal immune response that misses the target entirely and leads to the characteristic lung inflammation that has become a hallmark of the infection. What this means in practical terms, is that people who suffer wild-type infection often don’t mount great immune responses to the virus (reviewed here), and those responses seem to drop away with time. In other words, there may not ever be a population of truly immune people from this infection.
The only way to get immunity may be through an effective vaccine.
Both of the mRNA vaccine candidates, and other vaccines in development, have already worked to address this concern by demonstrating not only the typical antibody responses measured in most vaccine trials, but also effective T cell responses. This means that, on paper at least, we already have some reassurance that the immune response to this vaccine approach is meaningful and robust. In recent days, we have also learned that there is evidence of real-world protection for those who received the vaccine.
Both vaccine manufacturers have claimed around 95% “vaccine efficacy” from their vaccines. Now, this term has led to a lot of confusion, even among physicians, about what it really means. It does NOT mean that 95% of the subjects were protected. It also doesn’t mean that 95% of the subjects didn’t get the infection. It means that the risk of getting the infection was REDUCED by 95% compared to those who didn’t get the vaccine.
In real terms, the Pfizer numbers are a good example. Among the unvaccinated group, during the timeframe of followup (a minimum of 2 months) 162 patients were diagnosed with COVID. Among the group of vaccinated individuals over the same timeframe, there were only 8 infections.
The groups were randomized 1 to 1, meaning that approximately equal numbers of subjects should be in each group, and because the vaccine was randomly assigned the mix of ages, male/female, exposure risks etc ought to also be approximately equal between the two groups. So…one would also have expected around 162 infections in the vaccinated group, if the vaccine was not effective. Having only 8 infections is a huge decrease, which is where the “95% vaccine effectiveness” comes from.
What are the real world implications? There were over 43,000 patients enrolled, so approximately 21,500 would be in each group. 162/21500 is a rough guess of 0.75% of the population getting infected (although of course those people were enrolled over several months of time so the math is only a crude calculation). Those numbers mean that even without a vaccine, 99.25% of the placebo group didn’t catch COVID! I have heard arguments that the type of people who would enroll in a clinical trial like this may be more likely to wear masks and practice social distancing, which may be true, but if anything this would make it harder to detect a difference between the two groups, not easier – and the calculation of vaccine effectiveness doesn’t rely on knowing that. Nationally over the summer the average number of new cases in the US was about 50,000 a day. Over two months (approximately the average length of followup for the study participants, and the minimum required for safety data) that works out to 300,000, or about 0.9% of the total US population. This number is reassuring for two reasons – firstly it fits with the theory that the study participants were perhaps at a slightly lower risk of catching COVID compared to the national average, BUT the difference isn’t so great that it immediately calls the results into question. If the national rate was more like 10% and the study placebo rate was the 0.75% observed, it would look very suspicious. In theory, if the US population had been immunized over the summer instead of 50,000 cases a day, we would have had only 2,500 cases a day.
In addition, the safety data look great – significant fatigue and headache in 2-3% of the Pfizer participants after the second dose (I couldn’t find good data on the larger Moderna study, but the dose used in the Phase III study appeared to be well tolerated in earlier Phase II work). Now, admittedly we don’t have long term followup for several years because these vaccines are new, but intuitively and biologically we shouldn’t really expect any nasty surprises based on how the vaccine works in the body. One concern raised by some scientists and physicians is the possibility that the vaccine will induce an immune response that will make future infections worse – honestly, if that were the case we would have seen it in these clinical trial results. Among the “severe” COVID infections, in the Moderna study 0 of 11 cases were in the vaccinated group, and in the Pfizer study only 1 of 10.
So what do we have overall? We have a vaccine technology that induces biologically relevant immune responses that should be better than those of the real infection, with minimal risk. We have two clinical trials demonstrating dramatic differences between the vaccinated and unvaccinated groups that support highly protective vaccines. We have at best blunting of the epidemic from social distancing and masking, and an abject failure at containing it. Honestly, getting a COVID vaccine ought to be a no-brainer – it’s literally our last, best hope of getting back to something like normal, and it’s going to save millions of lives.
At the time of writing Dr Bennett has no financial conflicts of interest in any COVID vaccine product or company. He is a participant in a COVID vaccine study. Several of his friends have caught COVID (one was hospitalized), along with two non-immediate family members. Wear a damn mask.
