It’s taken me a little while to put virtual pen to paper in response to the appalling report from Reuters that revealed how an official US-government-sanctioned campaign set out to deliberately undermine COVID vaccination efforts in the Philippines.
Through phony internet accounts meant to impersonate Filipinos, the military’s propaganda efforts morphed into an anti-vax campaign. Social media posts decried the quality of face masks, test kits and the first vaccine that would become available in the Philippines – China’s Sinovac inoculation.
Reuters
The program, which apparently ran from 2020 through the end of the Trump administration and months into 2021, was a deliberate act of propaganda to undermine the influence of China on the global COVID vaccine stage (which the USA was not contributing to at all at the time). While Americans were “not targeted” by the misinformation, that specifically set out to disparage and undermine the Sinovac vaccine that was in widespread use in that region at the time, there cannot be any doubt that the lives of locals were placed at risk. As an infectious disease specialist who has dealt with antivaccine misinformation for all of their professional career, this is simply unacceptable to me. Regardless of the relative merits of one vaccine over another, or the petty machinations of the political regimes, during a global pandemic it is an abject failure of humanity to deliberately place other human beings in harm’s way.
This isn’t the first time that vaccines have been used as tactical tools – in the hunt for Bin Laden the CIA used a hepatitis vaccine program to collect DNA from children in an attempt to discover links to the terrorist in hiding. When the ruse became public, vaccine workers (even those with nothing to do with the program) were targeted and the polio eradication campaign stalled, with effects that have taken over a decade to even start to undo.
In response to the Pentagon’s efforts to undermine China, Filipino vaccine rates were woefully low, to the extent that the Government had to threaten jail for those who refused vaccination. When the US was approaching herd immunity at 65% coverage, in June 2021 the Philippines had only about 2% of their population immunized.
It takes a special kind of heartless disregard for science, and the welfare of other human beings, to promote this kind of act and go along with it. I suppose should we expect anything less, coming from a political leader who downplayed the seriousness and very existence of the problem and then politicized masking and social distancing, even as they sent protective equipment to their political allies. After vaccines became widely available, the anti-science mindset among Republicans was responsible for a 43% higher rate of excess deaths compared to Democrats in Florida and Ohio.
Arguably, deliberately undermining vaccine programs for political gain is tantamount to poisoning a water supply, which is literally a war crime. I cannot overstate how upset I am about this entire story – we as the experts have a hard enough time educating a scared and skeptical public about the measures that we are recommending to literally save them from themselves, without having our work attacked and undone by the powers that be.
A recent headline caught my eye, discussing an increase in the annual reported cases of Powassan virus – a virus which (for reasons that will become obvious) is near and dear to me. I decided to take a look at the actual data in more detail, and discuss a bit of that here, because understanding viruses like Powassan has implications beyond just this one infection.
Let’s start with what Powassan virus really is – it’s an arbovirus, meaning transmitted by arthropods (in this case, Ixodes ticks), and has an ability to cause a form of encephalitis. It is in fact closely related to the Tick Borne Encephalitis (TBE) virus, but Powassan virus was actually named after the town in Ontario where it was first discovered. It’s highly likely that many (perhaps the majority) of infections don’t go on to cause very serious disease, but the actual risk of encephalitis from it is unknown because the total number of cases isn’t really known. Of the symptomatic cases, about half are quite serious and 10% are fatal. The CDC has made it a nationally reportable infection, but the tricky part is knowing when to even think about it…
I diagnosed the first ever case of Powassan in Connecticut in 2016. It really was a bit of a crazy story, and truly a perfect storm of being in the right place at the right time. A young infant boy was admitted to the ICU with seizures and a very clear story of a few hours of a tick being attached to his leg 2 weeks earlier. The tick was brought into the house on a family member’s clothing, and probably got onto the child during a feed while being held by this person. The medical team had quite correctly ruled out most tick-borne infections due to the very short attachment time, but I knew that there was one exception – at least in animal models, Powassan virus could be transmitted in as few as 15 minutes. So it was possible, but was it probable? The clincher was the MRI report, which had a very distinct pattern showing “restricted diffusion of the basal ganglia and rostral thalami, as well as the left pulvinar”. There was no sign of more widespread of diffuse signal changes as you might see with ADEM (acute disseminated encephalomyelitis) or cerebellar changes as you might see with enterovirus. No hemorrhagic changes, as with herpes simplex. The laterality and location of the damage matched the physical symptoms (motor dysfunction affecting the right more than left), but more importantly it was also similar to previous reported scans from patients with arthropod-borne flaviviruses, including Powassan. Choi and Taylor wrote in a 2012 case report “MRI images of the patient’s central nervous system (CNS) were unique, and when such images are encountered in the clinical setting, Powassan viral infection should be considered.” We were able to test the baby’s spinal fluid at the CDC for Powassan, and it came back positive.
The points to make about this case are several – firstly, the recurring comment from most (probably all) of my colleagues when I made the diagnosis was “What made you think of it?” Honestly, it was mostly the fact that I had training in a state where Powassan was well-known and we would consider it routinely. I simply added it to the differential and saw that not only could I not rule it out, I had some evidence to support it! But the issue here is that there were probably many cases of Powassan over the years that doctors had been seeing, but simply never thought of testing. Powassan was not on a routine viral encephalitis panel in Connecticut (it’s a send-out to the CDC), whereas some other State laboratories like New York test for it automatically on their own encephalitis panel, in addition to sending/reporting to the CDC. It is very much a case of out of sight, out of mind.
Secondly, even if some physicians had considered and tested for the virus somehow, Connecticut didn’t make Powassan a reportable disease until 2019 (more than 2 years after I made the first diagnosis in the state). It’s really hard to measure something if you’re not counting it…and of course even hard to count something if you’re not looking for it!
So this makes it really, really hard to know what to do with news that “Powassan cases are increasing.” Reports are increasing, but so is awareness, and testing availability – it doesn’t mean that actual infections with the virus are going up. It is possible that they are…but the case reports alone aren’t enough to make that conclusion. You really have to understand the reporting infrastructure and testing limitations in the context of a specific disease when trying to interpret the changes you might see in any sort of incidence or prevalence data.
There isn’t a vaccine yet for Powassan virus, although when I last checked research was ongoing (and there is a vaccine for TBE). The best way to prevent infection is to avoid any kind of tick exposure at all – cover skin, use DEET, avoid tramping through the wilderness in areas where the virus is known to be in ticks, and check your pets! Also – change your clothing when you get indoors from activities that might have exposed you to ticks…
Bonus if you’ve made it this far – you can check out my TV appearance on Monsters Inside Me below!
I heard a little more recently on the contaminated blood scandal of the 1980s, where huge numbers of people with hemophilia were given treatments for their condition that were contaminated with viruses, including HIV and Hepatitis C.
Early on, there was little knowledge about the true risks of these viruses, and no proper testing available (certainly not widely available), but it turns out that some of this story is even worse than simply being given contaminated blood products.
An inquiry in the UK is currently focused on a specific series of infections that occurred at one particular school, which had a hemophilia treatment center on-site and which, it turned out, was also conducting research into novel treatments for the disease. At a superficial level the research seemed sound – it was asking the question: would a new heat-treated version of the clotting factors needed to treat hemophilia be safer than the standard treatments? Unfortunately, the heat-treatment wasn’t sufficient to completely inactivate the viruses – but the story is much worse than just that.
Several people have come forward who not only were infected with the viruses anyway, but possibly didn’t need treatment for their hemophilia at the time they were given the experimental treatments and, worse, neither they nor their parents were properly consented for the research. When the true risks of infection were obvious, subjects weren’t told, and some weren’t even informed of their infections for a year or more. One doctor involved in the study, a Dr Samual Machin (now deceased) is quoted during the inquiry:
“This would have been discussed with his mother, although I acknowledge that standards of consent in the 1980’s was quite different to what it is now,”
At the time, the subjects were all children, and several of the parents denied being properly told about the research, and that they would not have consented had they been told. Further documents showed that untreated patients were highly sought after, and that trying out the new heat-treated therapy may have been prioritized over the patients actual medical needs.
There are several core principles of research at stake here – beneficence (doing good), non-maleficence (do not do anything bad) and autonomy (being able to make your own decisions). Even a cursory look over the stories of this case show that none of those principles were upheld in this research, and of course the fact that the heat-treatment didn’t work to inactivate the viruses makes it all the worse (arguably if the research was a stunning success there wouldn’t be an inquiry into any of this…but that’s a whole other topic for discussion).
While there are regulatory rules for ensuring proper scientific conduct of research, there are also ethical rules. The two have some overlap, but they really are distinct frameworks, within which researchers have to function. The sad fact is that many of the rules and protections that we now take for granted were imposed as a direct consequence of past unethical human experimentation (which leads to another discussion about how what is considered “ethical” changes over time). From the perspective of human subjects and safety in particular, these are reflected primarily in the document we know as the ICF – the Informed Consent Form.
While it’s true that many aspects of subject safety, rights, and welfare are contained within the research protocol, the protocol itself is a highly technical description of the research and as more of a scientific justification and research plan. The ICF on the other hand is intended to be seen and understood by the study subject themselves, and includes a discussion on the research protocol (visits, procedures, timeline, risks etc.) in addition to making them aware of certain other rights afforded to them, including the right to leave the study at any time and any other treatment options available. The research site’s institutional review board (IRB) would have reviewed and edited the ICF to ensure that it accurately reflected the research risks and benefits prior to being seen by a potential subject. IRBs include subject-matter experts as well as members of the lay public to ensure clarity and understanding. Not only are potential study participants supposed to be given the opportunity to ask questions before signing the ICF, but they receive a copy and a copy remains in their medical record.
The fact that no such process occurred in these contaminated blood product studies is obvious.
Unfortunately, stories like this from research done decades ago, and which clearly doesn’t meet current standards, color everybody’s opinion of medical research. I have had parents refuse to consent for a study because “The sponsor is [insert drug company with research scandal] and I don’t trust them,” even though the drug in the study had nothing to do with the risks from the older scandal. I heard about one parent who turned down a study because of a poorly written ICF, that ironically overstated the risks in a summary paragraph that implied the drug had never been given to anyone before – some people might have continued reading, but this parent did not (they did however provide that feedback to the investigator, so we were able to modify the ICF to make it more clear). One time I had a sponsor try to avoid explaining all the risks (for the control therapy, not the study drug) in the ICF and instead provide a patient hand-out or “your doctor will explain this to you” verbiage. Despite our warning that the IRB would reject this ICF, they insisted on submitting it and of course wasted a whole IRB review cycle as they were forced to revise and resubmit the document with our recommended wording. This wasn’t an intentional thought to mislead, they genuinely thought it was a more efficient process and would avoid scaring the subject unnecessarily, but we knew that the ICF should be a stand-alone record of the subject being truly informed before consenting.
One of my experiences with obtaining consent sticks out to me – it was a slowly-recruiting antibiotic study and I was hoping to not have another screen-failure at my site. I had found a possible subject and was discussing the study with his mother and my study nurse. The mother was asking careful questions, clearly a little nervous (her son was in hospital after all!) and I was thinking that she probably wasn’t going to sign him up when she suddenly said “You know what, you’re the doctor and you know best, I’ll do whatever you say.” Massive red flag to me, as an investigator. Research isn’t the same as medical care – if “I knew what was best” we wouldn’t be having a conversation about a clinical trial! Also, if something were to happen during the study and she had rescinded the decision to me, then she as a mother would feel far worse than if she had made the decision truly believing she had made the best call. So I called “Investigator fiat” and screen-failed them. Every set of inclusion/exclusion criteria includes a line about “any other condition which, in the opinion of the Investigator. would interfere with the conduct of the study” and at that point I’m not sure that she fully understands the risks and benefits.
While we might celebrate some of these stories as holding ourselves to a high standard, the sad truth is the current standards of oversight and training that we have in medical research are much better than they were in the past mostly because of how poor they were in the past. Personally, I find it shocking that some of this occurred within my lifetime, and I think it behooves us to be mindful every day about how we conduct our research, placing the rights and welfare of our participants first.
It is a common misconception among physicians that engaging in medical research (or clinical trials) is not much different from practicing medicine – I’ve seen the question may times along the lines of:
“I’ve been asked to be an investigator for a clinical trial. How much work is it beyond finding patients, and how much will I get paid?”
There are so many aspects to this area that I’m actually going to devote several separate posts to this. I’ve thought for a long time that it would be a great idea to draft some educational material to help sites, subjects, and study staff to navigate the complexities that are clinical trials, and here we are.
I have been involved in clinical research for about 20 years now – covering everything from being a study coordinator recruiting subjects, collecting blood specimens, and completing case report forms, all the way through to being a medical monitor responsible for the safety of literally thousands of subjects, and ensuring that the data collected is as good as we can get. I have seen drugs fail, companies fall, and I’ve also seen new approvals get to market. It’s an incredibly rewarding career.
The art of medicine though requires a high level of insight and a degree of imagination – I have used a phrase along the lines of “Rules are for the protection of the weak and the guidance of the wise.” – usually right before I break a rule of some kind 😁. Physicians are in fact expected to think outside of the box and imagine what might be the diagnosis, and they have access to an ever-expanding arsenal of medical treatments to choose from for their patients (thanks to clinical trials – hint hint). Documentation is proscribed and expected, but the specific language used has considerable leeway. As strict as the framework of practicing medicine is, it’s still not that bad when you think about it.
Clinical Trials are a whole other beast. When an investigator agrees to oversee a clinical trial, they actually have to sign a legal document agreeing to follow a specific protocol for that study. This protocol isn’t just a plan to conduct the research – it is a highly detailed and specific document, with many ancillary documents, detailing every step of the subject’s journey from screening until closeout, and what might happen along the way. It is a document vetted by statisticians, clinical operations (people who work with the sites to execute the protocol), data managers, regulatory and legal experts, and independent physicians (protocol review is a routine part of a medical monitor’s job). The protocol has to be signed off by the FDA or other regulatory body at the country-level, so they agree that it doesn’t put subjects at undue risk and has all the required steps to meet the study objectives. As a simple example, enrolling too many subjects might put people at unnecessary risk, whereas enrolling too few subjects might make it statistically impossible to show that the clinical trial has succeeded. At the local level, every site has a Institutional Review Board (and sometimes a Scientific Review Board as well), and they also have to review and sign-off on the research as being appropriate. Everything that a subject might potentially see has to be vetted to ensure it is easy to understand, fully explains the risks and benefits of consenting to the research, and isn’t coercive. Every member of the study team has to have evidence of the proper training and qualifications to conduct not just research, but this protocol specifically.
Clinical research is so tightly regulated that an entire section of international (International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH) Guideline for Good Clinical Practice (GCP) ) and United States law (various parts of 21 CFR) is devoted to its conduct. The point being, that when an investigator agrees to conduct the study according to the approved protocol they cannot change it. They don’t get to chose when, or if, a subject shows up for a visit, they don’t get to chose the treatment (unless that is defined in the protocol), they don’t get to decide which tests are or are not performed – not unless there are very clear reasons and exceptions laid out. One obvious reason is for immediate subject safety needs, but that is exceedingly rare. I’ll talk more about Protocol Deviations and what they mean in a later post…
From the subject’s point of view though, I think it is crucial to appreciate that clinical research is by its very nature, and due to the scientific and and legal constraints placed upon it, incredibly strict and well thought-out. Clinical research is not a case of “let’s try this and see if it works”. I do think that subjects are aware of the second point about clinical trials – that they often provide access to new and as-yet unavailable treatment options. I know that the investigators are very mindful of this fact, and in truth one key motivator for being an investigator is in making these treatments available to their patients right away, and in contributing to the greater good by hopefully bringing a new treatment to market to make it available to all.
From the Investigator’s point of view, they should not undertake clinical research unless they are prepared to be held to an incredibly high standard – far higher than they are used to in the day-to-day practice of medicine. That is the price to pay for getting access to brand new and cutting-edge treatments. We’ll go over the specifics of the investigator’s role and responsibilities in a later post, but suffice to say – don’t do it for the money 😉.
*Tap tap* – is this thing still on? It’s been a while.
The recent slew of data coming out from Pfizer and Moderna about their respective COVID vaccines has prompted a LOT of discussion about their utility, safety, and efficacy. I’ve had friends and family hit me up for my opinion through social media, private messages, and phone calls, and the truth of the matter is there’s a 50% chance I’ve already got a vaccine, and if I haven’t the company is looking to provide it to those in the placebo arm. Yes, I’m in a COVID vaccine clinical trial – the science and need is compelling.
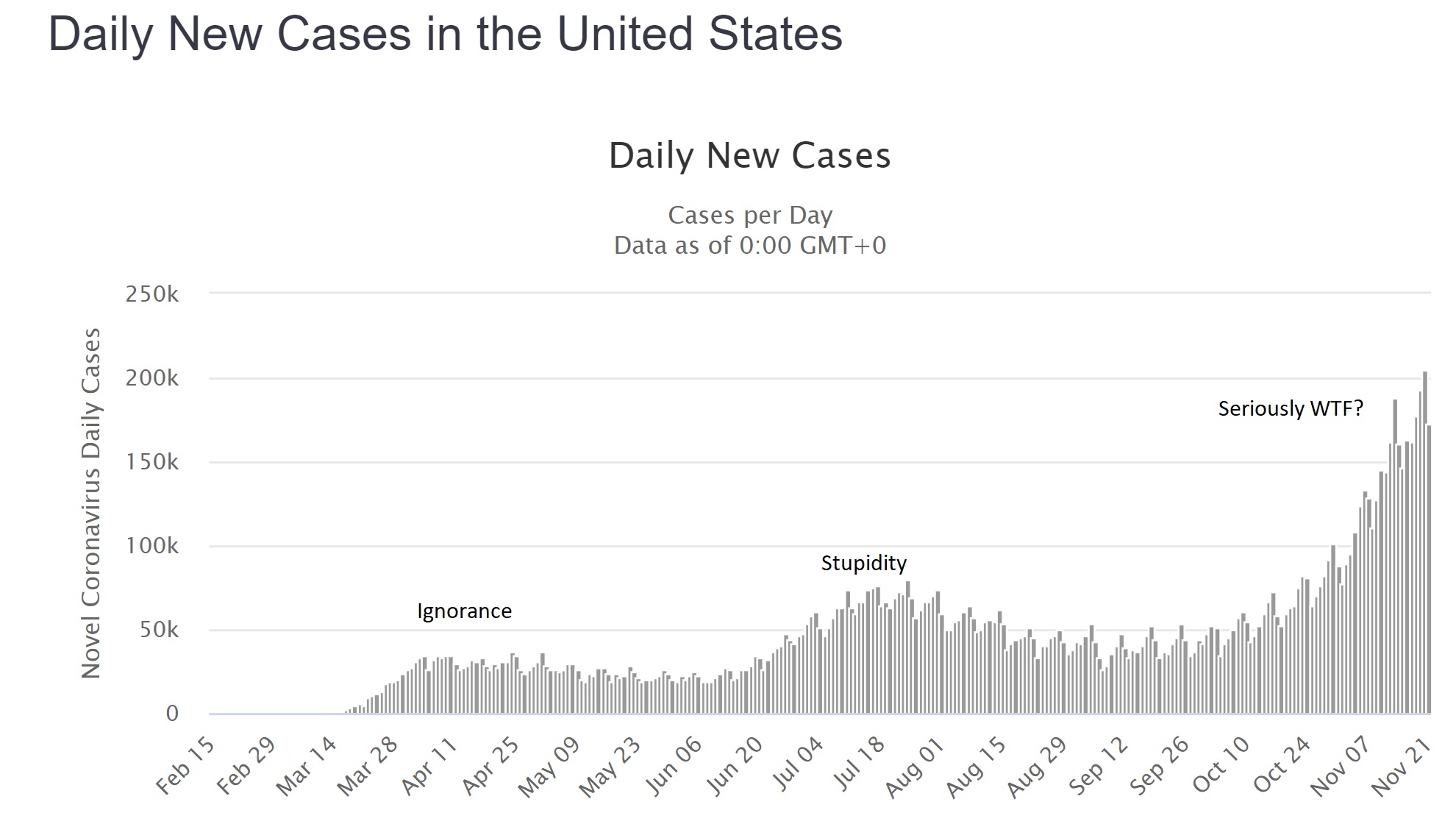
The global cases of COVID continue to climb with over 58 million worldwide as of today, of which about 12.5 million are in the US. Facing an accelerating “third wave” of cases of around 200,000 new reports and 2,000 deaths from COVID every day, there is no end in sight. This isn’t a hoax, it isn’t a “plandemic” or some other bizarre conspiracy theory, and it didn’t go away after the election – what we are dealing with is a predictable novel infection, likely zoonotic, the effects of which have been made worse by a series of abject failures in public health and education. I’m not going to debate that – it’s a matter of fact. Trolls will have their comments happily deleted, because I don’t argue with people who are wrong.
Having failed miserably to prevent the spread of this infection through such simple measures as staying home and covering faces, we now appear to have little option but to have faith in a vaccine of some kind. Herd immunity will otherwise cost millions of lives and probably trillions of dollars in lost productivity and economic output. The “low” mortality of 2-3% for COVID-19 is not low at all (the risk of death from a car crash is half of one percent, yet no-one in their right mind would recommend deliberately crashing their car…), and in any case the long-term effects of the infection on peoples’ health is likely to impact society for years to come. The fastest, safest way to stop the virus is through vaccination.
There are two vaccine candidates that have made headlines recently, both with similar technologies and claims of effectiveness, so for the sake of simplicity I’m going to talk about them generically. It seems likely that one or both of them will be approved by the FDA.
The vaccines use a “new” technology called “messenger RNA” or “mRNA”. The concept of an mRNA vaccine is not in fact new, and they have been researched for years. mRNA is entirely natural – every cell in your body contains some – very simply it is used as a go-between (a messenger…) from the genes coded within your DNA to the ribosomes where proteins are made. mRNA has a very specific structure – a linear molecule consisting of a mixture of 4 different nucleotides (adenine, cytosine, guanine and uracil) with a cap and a tail to ensure that the code is translated correctly and that other bits of RNA aren’t used accidentally. After the mRNA molecule is translated it is simply degraded and the individual nucleotides are recycled.
In theory, and apparently in practice, the use of an mRNA molecule as a vaccine would have several advantages. Most vaccines can be divided into one of two types: killed (or subunit) and live-attenuated. mRNA vaccines manage to combine the positive aspects of BOTH kinds, but the negative aspects of NEITHER. Allow me to explain.
In a normal viral infection the virus has to invade the body and evade the immune response, then infect a host cell. Viruses cannot replicate without a host cell, but in many instances the virus infection damages the cell function such that the host is affected and becomes sick. A virus that successfully infects a cell can take over the cellular functions, produce viral mRNA molecules, and force the cell to produce viral proteins. Cells though have several lines of defense, from producing chemicals called “interferons” that combat viral infection, to presenting viral antigens on their surface to the immune system (specifically, CD8+ T lymphocytes). Whether through the “innate” immune response like interferons, or through the “adaptive” immune response like T cells, nearly all of the time the host is able to successfully contain and clear a viral infection.
With a live-attenuated vaccine the goal is to mimic the natural infection, but without putting the host at risk of getting sick. The vaccine is usually made in such a way that the virus is defective and some aspect of its life-cycle is damaged – this means that the virus will still infect a cell and will still present its proteins to the host T cells, but the host simply won’t get as sick as they would with a wild-type infection. The result is often a VERY effective immune response that can last a lifetime after a single dose of vaccine, although sometimes boosters are given a few years later. Examples are measles, mumps, rubella, yellow fever, and oral polio vaccine.
Killed vaccines on the other hand use only “bits” of the virus, usually proteins that make up the capsid or outer membranes that are targets of the host immune response in natural infection. The hope is that by showing the host the purified proteins the immune system will produce a response that will recognize the virus should it try to infect the host in the future. The downside of these vaccines is that the type of immune response is slightly different, as the proteins are not presented from *inside* the cell. As such, the T cell responses are typically less, but instead there is a strong antibody response. Antibodies are very good at recognizing and neutralizing infections outside of cells, but of course since viruses replicate inside cells the real immunity actually depends on those CD8+ T cells. As such, killed vaccines often need multiple doses to be effective, and may not provide as much protection as the live vaccines would. Their advantage though is safety – there is literally no way for a killed vaccine to give the host an infection, whereas live-attenuated vaccines CAN cause disease if the host has an immune deficiency or if the virus mutates.
Looking now at mRNA vaccines it would seem as if they have the benefits of live-attenuated (internal protein production and presentation to T cells) AND the benefits of killed vaccines (no risk of causing infection in the host). In addition, despite the conspiracy theories you may read about online, there is no risk that the vaccine “becomes part of you” since there isn’t a mechanism for it to do so. Furthermore, a COVID-19 mRNA vaccine is an even better deal. The virus that causes COVID-19 has two very problematic aspects to it – firstly, it directly and significantly decreases that innate interferon response that is intended to stop the virus becoming established. This is likely because it evolved in bats, which have inherently high levels of interferon. In a human host, this virus is able to suppress our immune system very effectively, so that an otherwise mild infection is far more serious. Secondly, the adaptive immune responses (especially the T cell responses) in patients with COVID are also suppressed. Very early on it was obvious that the sickest patients with COVID had low number of lymphocytes, and over time we have come to realize that this also led to decreased adaptive immune responses against the virus. It seems that without the normal early response to infection, the host immune system is led awry, causing a dramatic, abnormal immune response that misses the target entirely and leads to the characteristic lung inflammation that has become a hallmark of the infection. What this means in practical terms, is that people who suffer wild-type infection often don’t mount great immune responses to the virus (reviewed here), and those responses seem to drop away with time. In other words, there may not ever be a population of truly immune people from this infection.
The only way to get immunity may be through an effective vaccine.
Both of the mRNA vaccine candidates, and other vaccines in development, have already worked to address this concern by demonstrating not only the typical antibody responses measured in most vaccine trials, but also effective T cell responses. This means that, on paper at least, we already have some reassurance that the immune response to this vaccine approach is meaningful and robust. In recent days, we have also learned that there is evidence of real-world protection for those who received the vaccine.
Both vaccine manufacturers have claimed around 95% “vaccine efficacy” from their vaccines. Now, this term has led to a lot of confusion, even among physicians, about what it really means. It does NOT mean that 95% of the subjects were protected. It also doesn’t mean that 95% of the subjects didn’t get the infection. It means that the risk of getting the infection was REDUCED by 95% compared to those who didn’t get the vaccine.
In real terms, the Pfizer numbers are a good example. Among the unvaccinated group, during the timeframe of followup (a minimum of 2 months) 162 patients were diagnosed with COVID. Among the group of vaccinated individuals over the same timeframe, there were only 8 infections.
The groups were randomized 1 to 1, meaning that approximately equal numbers of subjects should be in each group, and because the vaccine was randomly assigned the mix of ages, male/female, exposure risks etc ought to also be approximately equal between the two groups. So…one would also have expected around 162 infections in the vaccinated group, if the vaccine was not effective. Having only 8 infections is a huge decrease, which is where the “95% vaccine effectiveness” comes from.
What are the real world implications? There were over 43,000 patients enrolled, so approximately 21,500 would be in each group. 162/21500 is a rough guess of 0.75% of the population getting infected (although of course those people were enrolled over several months of time so the math is only a crude calculation). Those numbers mean that even without a vaccine, 99.25% of the placebo group didn’t catch COVID! I have heard arguments that the type of people who would enroll in a clinical trial like this may be more likely to wear masks and practice social distancing, which may be true, but if anything this would make it harder to detect a difference between the two groups, not easier – and the calculation of vaccine effectiveness doesn’t rely on knowing that. Nationally over the summer the average number of new cases in the US was about 50,000 a day. Over two months (approximately the average length of followup for the study participants, and the minimum required for safety data) that works out to 300,000, or about 0.9% of the total US population. This number is reassuring for two reasons – firstly it fits with the theory that the study participants were perhaps at a slightly lower risk of catching COVID compared to the national average, BUT the difference isn’t so great that it immediately calls the results into question. If the national rate was more like 10% and the study placebo rate was the 0.75% observed, it would look very suspicious. In theory, if the US population had been immunized over the summer instead of 50,000 cases a day, we would have had only 2,500 cases a day.
In addition, the safety data look great – significant fatigue and headache in 2-3% of the Pfizer participants after the second dose (I couldn’t find good data on the larger Moderna study, but the dose used in the Phase III study appeared to be well tolerated in earlier Phase II work). Now, admittedly we don’t have long term followup for several years because these vaccines are new, but intuitively and biologically we shouldn’t really expect any nasty surprises based on how the vaccine works in the body. One concern raised by some scientists and physicians is the possibility that the vaccine will induce an immune response that will make future infections worse – honestly, if that were the case we would have seen it in these clinical trial results. Among the “severe” COVID infections, in the Moderna study 0 of 11 cases were in the vaccinated group, and in the Pfizer study only 1 of 10.
So what do we have overall? We have a vaccine technology that induces biologically relevant immune responses that should be better than those of the real infection, with minimal risk. We have two clinical trials demonstrating dramatic differences between the vaccinated and unvaccinated groups that support highly protective vaccines. We have at best blunting of the epidemic from social distancing and masking, and an abject failure at containing it. Honestly, getting a COVID vaccine ought to be a no-brainer – it’s literally our last, best hope of getting back to something like normal, and it’s going to save millions of lives.
At the time of writing Dr Bennett has no financial conflicts of interest in any COVID vaccine product or company. He is a participant in a COVID vaccine study. Several of his friends have caught COVID (one was hospitalized), along with two non-immediate family members. Wear a damn mask.
For those who haven’t been under a rock recently, several parts of the US have seen a surge in pertussis cases. Much of this has been (fairly) blamed on anti-vaccination efforts to reduce herd immunity and the cocooning of vulnerable infants. But that’s not the whole story.
Interestingly enough, it’s now clear that the DTaP vaccine (diphtheria, tetanus, acellular pertussis) doesn’t provide long-lasting immunity. We had some clues with this as an awareness grew of pertussis in older teens and adults, fueled in part by vastly improved testing for pertussis (PCR versus ‘cough plates’ for culture) and a recognition that pertussis in older kids and adults didn’t look like the classic ‘whopping cough’ that youngsters got.
A booster dose of pertussis vaccine was recommended, included as part of the tetanus booster (the new Tdap vaccines). Recent outbreaks seemed to focus on the group of kids aged 10-11 years of age – when vaccine immunity was waning, but just before their Tdap booster – but the recent outbreak in Washington State has involved even 13-14 year olds, who did get their booster!
The question then should be – why does the NEW vaccine work LESS well? The answer is because it is SAFER.
The old DTP vaccine began to get a bad reputation for neurologic disease – in fact a contraindication still exists to withhold pertussis-containing vaccines in kids who develop neurologic issues after pertussis vaccination, even though the vaccine is different. The old DTP contain literally thousands of antigens, based as it was on a relatively impure cocktail of cell culture fragments that contained the pertussis bacteria. It caused a fair amount of immune reaction, and clearly was linked to febrile seizures.
Several high-profile cases of apparently neurologically damaged children (leading to the formation of some of the early modern anti-vaccine movement) pushed the vaccine manufacturers to create a cleaner vaccine, an ‘acellular’ pertussis vaccine, which is why we have DTP and DTaP. DTaP doesn’t have the same link of febrile seizures and no link to any neurologic issues (interestingly, as detailed in Paul Offit’s book on the history of antivaccine junk science, neither do any of the original DTP kids…it was all a big screwup). Tdap is even less immunogenic as it has slower concentration of antigens – you can tell this because it has a small “p” instead of a big “P”. True story.
The trouble of course is that by having a less inflammatory response, with far fewer antigens, the protection is less. The original DTP vaccine contained more antigens than the ENTIRE modern vaccine schedule does, several times over. Any statement about ‘too many too soon’ is pure bunk – our kids are exposed to fewer vaccine antigens in their entire schedule that we were in one vaccine.
This story highlights several points – firstly, contrary to antivax propaganda, not only are there mechanisms in place to detect and respond to potential vaccine side effects but there are CHANGES made to the vaccines in an attempt to keep people safe. (Probably the only positive thing to come out of the antivax movement is the establishment of the Vaccine Adverse Event Reporting System, VAERS). Secondly, there are compromises to be made – more effective sometimes also means more side effects, so if you want to lower one you may end up lowering the other.
There is also data from Europe that as the vaccine strains of pertussis wane, there is strain replacement with potentially more virulent strains. So although we are seeing fewer cases, those cases we do see may be more serious (this finding hasn’t yet held true for the US…as far as I know).
Sadly, those who believe antivax propaganda are not usually stupid – if anything they tend to be more educated than average, and well read. They just read the wrong things. Not everyone can go to medical school after all.
Then again, even that isn’t foolproof. One of the original antivax “Expert” witnesses from the UK trials that showed the DTP link with neurologic illness to be wrong went on to further his infamy with AIDS denialism.
Much of the details on the stories of the DTP and DTaP history are in Paul Offit’s book – Deadly Choices, which I highly recommend. In it he not only details how antivax proponents twist science and the facts to suit their case, but also how they nearly brought down the entire US vaccine industry through irresponsible and indefensible litigation. The vaccine WORKS to reduce serious illness from pertussis and undoubtedly saves lives. It’s not perfect, no one has ever said a vaccine was perfect – at least, not unless they were trying to make a point that it wasn’t…
Just for a moment I’m going to take the view that vaccines are, you know, safe and effective. Sure, there are known side effects, mostly mild short-lived things like injection-site reactions or fever, but Bad Things do happen (e.g. Vaccine Associated Paralytic Polio from the live oral polio vaccine). On balance though it is clear that the benefits of vaccination to society as a whole outweigh the risks to society as a whole. Their success is measured in what we DON’T see – the 20,000 HiB cases a year, the 80-90% drop in pneumococcal disease from vaccine strains, the congenital rubella cases that every medical student knows how to spot (“Blueberry Muffin” baby, cataracts, persistent ductus arteriosus) but will likely never see in their professional lifetime. Safety monitoring is there, as imperfect as it is, which is why for example we don’t have oral polio vaccine in the US any more, and why the first rotavirus vaccine was pulled from the market.
So if we were to take a purely logical view on the matter, vaccination is a no-brainer. For many Docs this is why they get so irate about vaccine refusers. We learn about the diseases and the successes, and find it hard to fathom how you could come to any different conclusion. But clearly people do. There are unfounded fears about “too many too soon”, or aluminum adjuvants that add less exposure than breastmilk, or the fraudulent claim of autism causation that ended up being a scam for one Doc (the infamous Andrew Wakefield) to sell his own measles vaccine. Some parents are simply worried based on a previous bad reaction (I know I was, based on the way my eldest acted after his 2 month shots). Others have a genuine religious belief about medical interventions, and vaccination is just one aspect of that.
So then we run up against the problem of how to deal with this issue. As a general rule of thumb, it is accepted that a patient has the right to refuse aspects of their healthcare. There are very few exceptions to that rule, usually in the interests of others in society – forced hospitalization of mentally ill people who pose a threat to themselves or others, or cases of medical neglect where the State assumes responsibility for the medical decisions of a child when the parent puts them at risk, or Directly Observed Therapy for TB, where optimal treatment is paramount and doses should not be skipped. Things like that.
But vaccines are put into a different category. Why? I think the biggest, most obvious difference is that we’re not talking about treatment of someone with a disease, where inaction has obvious consequences, but rather an intervention to a typically healthy individual. In fact, moderate illness (enough to require hospitalization) is one reason to consider delaying vaccination, as the immunization might not work as well. As such, even though the results of inaction can be severe, resulting in death or disability, and inaction certainly has an impact on others in society, there is a natural reluctance to literally force vaccination upon people. Instead, there are more insidious ways to encourage vaccination through school mandates etc. Vaccines are not mandatory, you just have to get them. (If you can understand that, let me know, as that was how a non-mandatory examination was explained to us in medical school…)
As one approach, I am going to use the analogy of rabbits. Above you can see Princess Lulu Merryweather, an Old English Mini-Lop who was with us for over 8 years before succumbing to a pasteurella abscess. Lulu was a house rabbit and was pretty much housetrained. She knew a basic list of commands and would poop in her cage. The training of a bunny is interesting – as a prey animal they do not respond well to the typical training one might use with a predator animal such as a dog or cat. They are more like a horse, and respond best to coercion rather than discipline. In fact, an effective way to get them to do what you want is to embarrass them. This is difficult to do. It generally involves stamping your foot, turning your back on them, but trying to make eye contact so you know that they know that you are displeased. If you’ve ever had a bunny and told them off for something, you’ve probably seen them do this to you. There were several occasions when, as a kitten, she would pee on the couch and we would both end up stamping and back-turning on each other as I would tell her not to do that, and she would try to tell me not to shoo her off the couch. It was her couch, after all. (Did I mention the “Princess” part was added later? It was more a description than a title…)
So, since the decision not to vaccinate is often based more on emotion than logic, it seems reasonable that for some people (not all of course) an emotional approach will work better than a logical one. Human beings are hard-wired to fear bad things from an action (to vaccinate) more than from inaction (not vaccinating), even though a decision to do nothing is still technically a decision, and fear after all is an emotion. I wonder then if pressure from society, an explicit message that says that unvaccinated kids are an unacceptable risk to others would work. Peer pressure. At the moment we have an attitude of tolerance on the whole – barely more than a raised eyebrow, more often a nod of understanding. There may be pressure from the Docs and schools who are trying to protect society from itself, but there needs to be a grass-roots movement among the parents in my opinion.
I’m not entirely sure yet how exactly to go about doing this. I don’t agree with literally holding a parent back while we forcibly inject their child – since after all we do live in an age where many of the preventable diseases are at very low levels, and that goes against every fiber of my “patient-centered” being. I would much rather have informed decision-making – I just realize that for many their mind is made up no matter what facts I lay out and what misconceptions I correct. What I would like to see is an attitude of personal responsibility to temper the push for personal freedoms. Parents should WANT to vaccinate. Currently most fall into the “I don’t care” or the “I don’t want to” camps. That kind of paradigm shift may be slow coming, and I’m open for suggestions on how that might occur. We can’t use a stick, we need to use the carrot.